Histamine Intolerance: A Gut–Vagus–Mast Cell Story
"Histamine intolerance" is one of the most over-simplified diagnoses in functional medicine. The popular framing — too much histamine, not enough DAO enzyme — captures a fraction of the picture. The clinical reality is a three-way conversation between the gut, the vagus nerve, and the mast cell. When all three are calm, histamine is metabolized invisibly. When one fails, the others compensate poorly. When two fail, the patient develops symptoms.
The DAO Enzyme: Necessary, Not Sufficient
Diamine oxidase is a copper-dependent enzyme that breaks down histamine in the gut and kidneys (WebMD overview). DAO insufficiency raises the histamine load arriving in circulation. But DAO levels alone do not predict symptoms — many patients with normal DAO have classic histamine reactivity, and many patients with low DAO are asymptomatic.
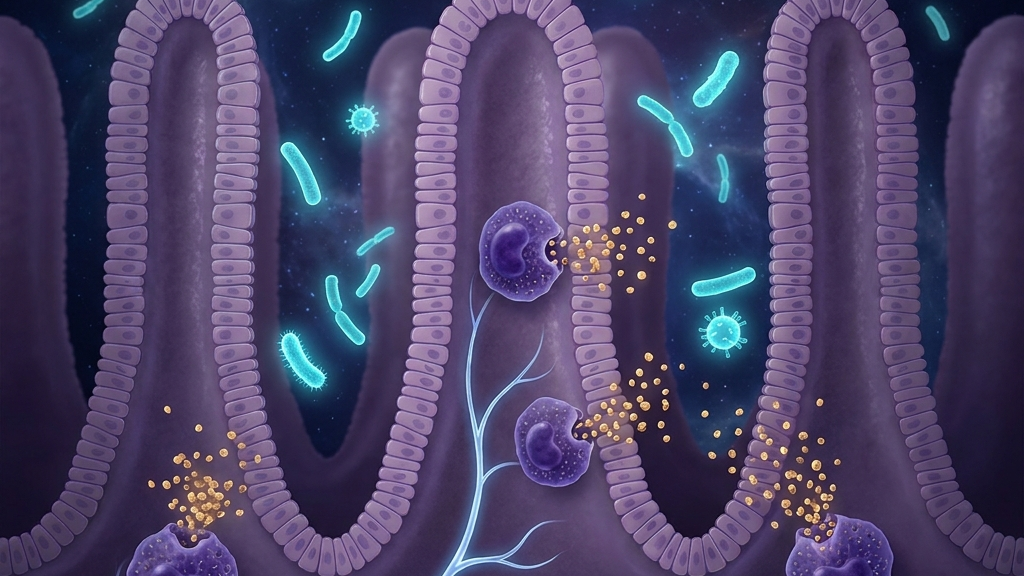
The Gut Is the Real Engine
The dominant source of histamine in many "intolerance" patients is not dietary — it is microbial. Several common gut bacteria produce histamine through histidine decarboxylase (PMC 8069563). In SIBO, dysbiosis, or post-infectious gut states, histamine output rises sharply within the gut lumen — often outpacing DAO clearance.
A 2022 pilot study showed that targeted dietary intervention reduced the abundance of histamine-secreting bacteria and improved symptoms in histamine-intolerant women (PMC 9633985). The microbiome is not background — it is the engine.
The Vagus Nerve as the Gatekeeper
Vagal afferents sense gut histamine levels and visceral inflammation. Vagal efferents release acetylcholine, which binds α7 nicotinic receptors on mast cells and suppresses degranulation. When vagal tone drops, mast cells become more reactive — and the same dietary load that was tolerated yesterday triggers a reaction today. Many patients describe this clearly: "It is not the food. It is what I am when I eat the food."
The Patient Profile
Classic histamine intolerance presents with: flushing, headaches after fermented foods or wine, runny nose with no allergies, GI cramping or loose stools, hives, sleep disturbance, palpitations, brain fog, and reactivity to fragrances. Typical comorbidities include SIBO, IBS, MCAS, hEDS, and POTS — the same autonomic-immune cluster recurring across diagnoses.
A Three-Layer Treatment Framework
Layer 1: The Gut
Address dysbiosis, SIBO, and intestinal permeability. A short low-histamine diet can buy symptomatic relief while microbiome work proceeds — but indefinite restriction is not the goal.
Layer 2: Mast Cell Stabilization
H1 + H2 antihistamines, quercetin, vitamin C, and — where indicated — cromolyn or ketotifen. DAO supplementation around meals can help selected patients.
Layer 3: Vagal Tone
This is the layer most often missed. Slow nasal breathing at six per minute, cold-water face immersion, consistent sleep, and — where appropriate — auricular taVNS. Practices that support vagal tone meaningfully reduce mast cell reactivity even before any dietary or pharmacological change.
Clinical takeaway: Histamine intolerance is a symptom, not a diagnosis. The durable answer lives in the gut, the mast cells, and the vagus nerve — not in any one of them alone.
References & Further Reading
Have a question?
Have a question about something specific? Send us a message.
Visit VagusSkool.com/contact — we'll try to get back to you within 24 hours.