Auricular Vagus Nerve Stimulation — The Ear as a Gateway to the Brain
Auricular Vagus Nerve Stimulation — The Ear as a Gateway to the Brain
Thesis
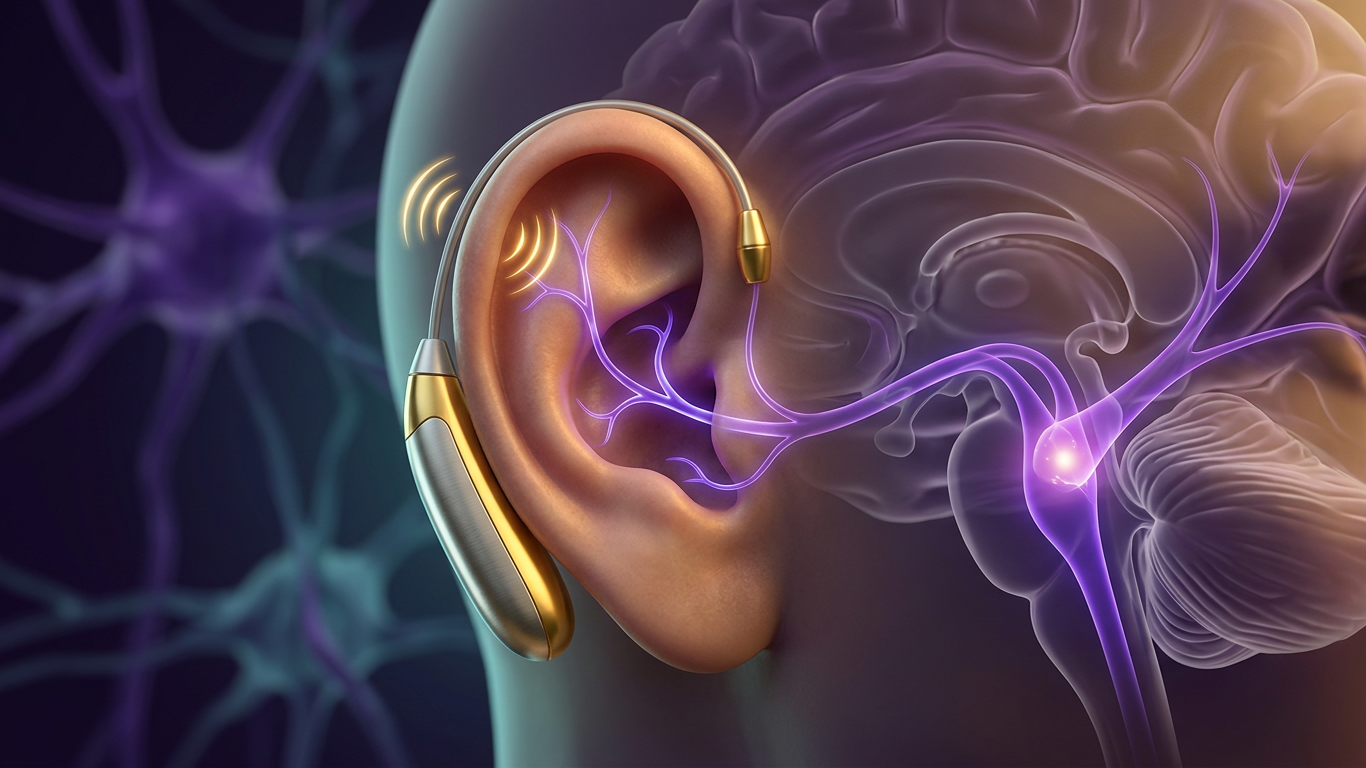
Your ear has a direct line to the brainstem — through the auricular branch of the vagus nerve (Arnold's nerve). The cymba concha of the outer ear is innervated by the vagus nerve in 100% of anatomical dissections, making it the most reliable non-invasive access point for vagal stimulation. At just 1–1.5mm depth beneath the skin, targeted electrical stimulation of this region activates brainstem nuclei that regulate inflammation, mood, pain, and autonomic function — all without surgery.
Key Questions
- Where exactly does the vagus nerve innervate the ear, and what are the optimal stimulation sites?
- What fiber types carry auricular vagal signals, and what thresholds are needed?
- How does auricular VNS compare to cervical VNS for therapeutic effects?
- What clinical conditions respond to ear-based vagal stimulation?
Supporting Research
Kaniusas, E. et al. (2019). Current Directions in the Auricular Vagus Nerve Stimulation I — A Physiological Perspective. Frontiers in Neuroscience, 13, 772.
DOI: 10.3389/fnins.2019.00772 | PMC
Ear Anatomy and Vagal Innervation
The auricular branch of the vagus nerve originates from the jugular ganglion and enters the ear centrally. Based on dissection studies, the innervation prevalence varies by region:
- Cymba concha: 100% — exclusively vagal, the optimal stimulation site
- Central concha: Mostly (high percentage) vagal
- Antihelix: 73% vagal innervation
- Cavity of concha: 45%
- Tragus: 45% (commonly used for transcutaneous aVNS but less selectively vagal)
- Crus of helix: 20%
The ear lobe, spine of helix, and upper medial auricle are NOT primarily vagal — they're innervated by the great auricular nerve, auriculotemporal nerve (trigeminal), and lesser occipital nerve respectively.
Fiber Types and Stimulation Thresholds
The auricular vagus nerve contains approximately 370 myelinated axons per ear, plus unmyelinated fibers:
- Aβ fibers (myelinated, 7–10μm): ~20% of myelinated axons. Low-threshold sensory. Activate at 5–7x detection threshold.
- Aδ fibers (myelinated, 2–5μm): ~50% of myelinated axons. Nociceptive (pain sensing).
- C fibers (unmyelinated, <2μm): Majority of total fiber population. Polymodal nociception.
Effective stimulation targets Aβ and Aδ fibers while avoiding noxious C-fiber activation. This means moderate, comfortable stimulation intensities — not painful ones.
The Afferent Pathway
When auricular vagal fibers are stimulated, signals travel to the nucleus tractus solitarius (NTS) in the brainstem. The NTS then projects to:
- Locus coeruleus: Norepinephrine release → arousal, attention, neuroplasticity
- Dorsal raphe: Serotonin modulation → mood regulation
- Amygdala: Emotional processing and fear extinction
- Hypothalamus: HPA axis regulation, autonomic balance
- Dorsal motor nucleus: Parasympathetic efferent output → anti-inflammatory cholinergic pathway
Clinical Applications
- Epilepsy: First FDA-approved indication for auricular VNS
- Depression: Transcutaneous auricular VNS shows antidepressant effects comparable to cervical VNS
- Pain management: Activates descending pain inhibition pathways
- Inflammation: Stimulates the cholinergic anti-inflammatory pathway
- Heart rate variability: Increases vagal tone and HRV indices
Why This Matters
Auricular VNS democratizes access to vagal stimulation. Cervical VNS requires surgery (implanting electrodes on the vagus nerve in the neck). Auricular VNS can be performed with surface electrodes, ear clips, or even smartphone-controlled devices. The cymba concha — sitting right there on your ear — is a 100% reliable vagal access point that requires no incisions, no anesthesia, and no hospital visit.
Experimental Predictions
- Stimulation at the cymba concha should produce stronger brainstem activation than stimulation at the tragus
- Aβ fiber-selective stimulation (below pain threshold) should produce therapeutic effects without discomfort
- Chronic auricular VNS should show cumulative improvements in baseline vagal tone
- Combining auricular VNS with resonance frequency breathing should produce synergistic autonomic effects
Have a question?
Have a question about something specific? Send us a message.
Visit VagusSkool.com/contact — we'll try to get back to you within 24 hours.